|
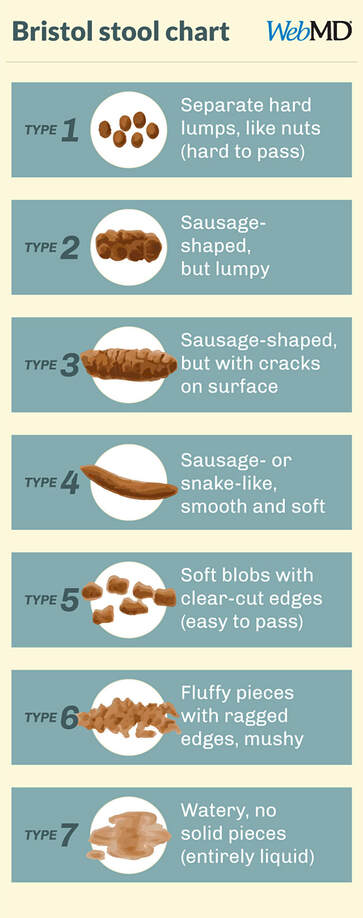
It’s really common for toddlers and preschoolers to have trouble pooping, and I am frequently asked about how to resolve children’s constipation. It can be emotional and exhausting for all involved - the upset, the denial, the hopping and wiggling, the lethargy and low appetite. This has come up again recently (including with my own kids!) during quarantine, and there’s a couple of reasons that might be: change from our regular routine, different foods due to reduced availability, lower activity levels due to stay-at-home orders, and maybe some household stress in the mix too. I’m going to run through some of the reasons that kids have trouble going to the bathroom, some of the pitfalls to avoid, and some of the solutions. Fair warning, there is lots of poop talk ahead!
|
AuthorHi, I'm Amy. I'm a nutritionist in the DC area, working with clients of all ages, focusing on prenatal and pediatrics. I'm all about straightforward, evidence-based health & wellness advice - because life/parenting in the modern world is complicated enough! Categories
All
November 2022
|
Seed to Sapling Nutrition



 RSS Feed
RSS Feed