 Parents need information, not judgement All parents want to give their babies the best start in life, and nutrition is no exception. Breast milk or formula should be the sole source of nutrition for infants under six months, and should remain the primary source of nutrients until at least 12 months (AAP). While most mothers (83%) in the US start out breastfeeding their babies, less than half are exclusively breastfeeding at three months, and only 25% are breastfeeding exclusively at six months (CDC). This tells us that most families are looking for alternatives to supplement or replace breastmilk within the first six months. There is no shame in this – modern motherhood is HARD! We have virtually non-existent maternity leave in the United States (the only developed nation that doesn’t offer federally mandated paid parental leave), making it more logistically challenging to breastfeed our infants. With around a third of babies being born via C-section, many women don’t have the opportunity to nurse their babies during the first hour after birth, which plays a role in breastfeeding success. And, with complicated deliveries, mother or baby (or both) are busy being treated for complications, or sleeping off meds, so things don’t always get off to the best start. Structural and societal support are also lacking, with only 25% of babies born in hospitals that provide an optimal level of support for lactation (the Baby Friendly designation from WHO and UNICEF guidelines); while this is a significant improvement from a decade ago (only 3% in 2007; BabyFriendlyUSA), it's still not optimal. Plus, in the US we also face a taboo around breastfeeding in public which adds an additional barrier to success. Some women experience low milk supply, or a baby who struggles to latch, or a colicky baby who never seems satisfied. These are things that a lactation consultant can help with, and smooth the (often bumpy) breastfeeding journey, but not everyone has access to one at the right time, place, or price point. Some women are plagued with self-doubt and/or exhaustion at 3 am, or a well-meaning loved one tells them to sleep through the night while they feed the baby, and that little bottle of formula that the hospital sent you home with (“just in case”) is readily available. Some women commit to breastfeeding exclusively for the first six months, then choose to switch to formula for the rest of the first year, and other women decide from the get-go that they won't be nursing, as is their prerogative. Women KNOW that breastfeeding is optimal, and they may have a whole bunch of feelings around the fact that they’re not doing it as much or as long as they'd like - they simply want to know what the best substitute is if they decide that need one. Whatever their reason, most women do not come to the decision to stop nursing lightly and deserve our support in choosing the next best thing for their child. What are the options?
Commercial formulae, deep dive: Plant-based formulae are non-dairy alternatives for babies who struggle with cows’ milk-based formulae and/or families who choose a vegan lifestyle. Soy formula has fallen out of favor recently: most soy in the USA is genetically modified (94%, 1), which is a concern for many parents due to pesticide exposure. There have also been concerns that exposure to high levels of phytoestrogens naturally occurring in soy could be harmful to babies, particularly girls in later life (2). In response to these concerns, the National Toxicology Program's Center for the Evaluation of Risks to Human Reproduction (CERHR) convened an expert panel to evaluate soy infant formula in 2009 and concluded that there was minimal concern for babies drinking soy–based formulae. Regardless, many parents would rather not give their babies controversial ingredients, and a recent newcomer to the market place uses pea protein as an alternative. Organic vs. Conventional: choosing organic means skipping the pesticides, herbicides, and growth hormones that are often present in conventional milk and soy products. That being said, the USA has an increasingly long list of ingredients that are permitted in products certified organic, some of which are from dubious sources. Another designation worth looking out for, in the absence of organic certification, is non-GMO project verified. While GMOs are banned in Europe, in the USA they are generally regarded as safe. GMOs are exposed to higher than normal levels of pesticides and herbicides, toxins which infants’ immature systems have a harder time clearing. There is some observational evidence of a link between exposure to pesticides in utero and infancy and increased incidence of autistic spectrum disorders (3). With studies showing that eating organic does effectively reduce levels of pesticides in our children’s bodies (4), it is worth the extra cost, if you can afford it. Types of fats, including DHA & ARA: the omega-3 fatty acids in breastmilk are one of its selling points, thought to be responsible for boosting babies’ brain health. DHA is a key building block for your baby's brain and eyes, and formula-fed babies have been shown to have lower levels, so it is only natural that manufacturers want to add this to their products. However, most US manufacturers use DHA from algal oil, which is somewhat controversial due to processing methods, plus the benefits of adding this as an isolated ingredient are not well established. The FDA has now expressed some concerns about adding it to formula since approving it in 2002 (5). Artificial ARA and DHA will show up as m. alpina oil and c. cohnii oil in the ingredients list. Some complain that it is synthetic and uses known neurotoxins in processing, therefore shouldn’t be added to any products labelled organic, but it is on the aforementioned list of ingredients that get a pass. Good quality European brands use fish oil as their source for added fatty acids, while some in the US use DHA from eggs. Aside from the omega-3s, the sources of fats in formulae usually include a mix of plant-based fats such as coconut oil, soy oil, canola oil, sunflower oil, and palm oil. Formula is typically slightly lower in fat than breast milk (and slightly higher in carbs and protein). Types of carbohydrate & sugars: breast milk contains lactose, a natural sugar, and complex carbohydrates called human milk oligosaccharides (HMOs) which work as prebiotics – food for the developing microbiota in the babies’ guts. HMOs play a significant role in establishing immune and gut function and protect against pathogens (6). Some formula companies are now adding synthetic HMOs to their products, and industry-sponsored research suggests that this conveys some health benefits (7). Most commercial formulae in the US use simple sugars such as corn syrup, glucose syrup (often from wheat) and sucrose; these are probably from GMO sources unless certified otherwise (look for non-GMO or certified organic). Sucrose isn’t great for teeth, so once baby has a few, you may want to clean their teeth after feeding them formula containing sucrose. Some of the organic brands opt for brown rice syrup instead of other sugars, but brown rice syrup can have high levels of arsenic – one study found that baby formulae with organic brown rice syrup had 20 times the arsenic levels of those formulae not using it (8). Maltodextrin is another controversial additive: a long chain carbohydrate derived from corn or wheat, it can disrupt the gut microbiota, which isn’t what we want during such a critical period of microbiome development (9). Iron: adequate intake of iron for an infant 0-6 months old is 0.27 mg/day; for a 6-12-month-old this jumps to 11 mg/day. Babies’ needs actually increase gradually as the months go by, due to dwindling iron stores (babies stock up in utero, assuming the mother is well-nourished, and the pregnancy is full term). Infants start eating solid foods around six months, which provide a source of iron in their diet. It is worth noting that iron is one of the nutrients where more is not better, in fact, more can be harmful, so we should always supplement with caution. It used to be possible to buy both low iron and high iron formulae (typically 4 mg/L vs. 11 mg/L), but now low iron formulae are harder to find in the US. Lower iron is usually adequate for younger babies (10). If we are looking to nature for our model, mothers’ milk has very low levels (0.5 mg/L), and full-term healthy babies are born with enough stored iron to last the first 4-6 months (or longer if they didn’t have their umbilical cord clamped immediately at birth). Additionally, it takes the gut around six months to mature, and during this time it does a poor job of regulating iron uptake, meaning that a lot of the supplemental iron sits in the developing GI tract, where it may cause constipation and increase susceptibility to GI infections, as well as interfering with absorption of other minerals. High iron formulae are the norm in the US, with almost all brands having ~12mg/L; for comparison, most European brands stick with <7 mg/L, especially for younger babies. It is worth restating that the RDA for younger infants is 0.27 mg/d, which this far exceeds. One of the reasons for this is that the iron in breastmilk is very well absorbed due to an iron-binding protein called lactoferrin, which nature provides to ensure absorption of the naturally occurring iron in breast milk – around 50% of iron from breast milk is absorbed, vs. 7-12% of supplemental iron in formula. Some formula companies add bovine lactoferrin to their formulae to aid with absorption, but there are mixed results about whether this is beneficial. Probiotics: The live cultures in breastmilk are one of the keys ways in which it is ‘better than’ human milk alternatives. Research has shown that breast milk contains over 700 different types of bacteria, including common probiotic strains such as Lactobacillus and Bifidobacterium, as well as Streptococcus, Staphylococcus and Enterococcus. The breast milk microbiota shifts continuously to meet the ever-changing needs of the infant: over the first few months of a baby’s life the concentration of different strains of microbes in their mother’s milk shifts from month to month, and during each nursing session the baby’s saliva transmits information on its health status to the mother’s immune system, allowing for customized defenses at the next nursing session. Because of this, human milk probiotics are not truly replicable, but adding probiotics to formula certainly makes sense, as formula-fed babies are otherwise missing out on this key element of gut and immune development. Probiotic supplements are emerging as a potential way of alleviating colic (e.g. L. Reuteri), and reducing allergies and atopy in infants (e.g. LGG and L gasseri). It might make sense to supplement your baby with these if they're prone to these conditions, but you don't necessarily need it to be in their formula, you can supplement separately with whatever is best suited to your child's needs. Lactobacillus infantis is an important strain that babies get from their mothers during vaginal birth, associated with reduced intestinal inflammation, but recent findings from a probiotic company studying baby poop found that up to 90% of US infants have no L. infantis in their microbiome (11). This is probably due to the increase in c-section deliveries and the use of antibiotics in early life, across generations - if mom doesn't have these microbes, she can't pass them on to her infant. Formulae of the future will likely have many more added as we learn more about the human milk microbiota. That being said, for now it is probably more useful to supplement with a separate multi-strain probiotic that meets the unique needs of your child (e.g. colicky, or risk of allergies, etc), rather than going with a formula advertising that it has added probiotics but usually only has one or two strains. BPA: a plasticizer used in hard plastic bottles and for lining cans, this chemical can leach into liquid formula preparations, but it doesn’t appear to leach into powdered formulae. When it comes to feeding your baby, stick with glass baby bottles to reduce BPA exposure further – bottle-fed babies (whatever they’re drinking) are exposed to more BPA than babies fed at the breast. If you must use plastic bottles (some daycares ban glass), be mindful not to heat them, and hand-wash them to reduce leaching. Water quality: if you are mixing powdered formulae with water, you’ll want to be sure that the tap water in your area is safe to drink. A recent report from the EWG (12) found that 97% of water samples from across the USA were contaminated with PFAS – industrial chemicals that never breakdown, and have been associated with various health concerns (13). This is far more widespread than previously believed. Also, the CDC cautions against regularly mixing formula with fluoridated water, because excess fluoride can discolor emerging teeth. About 70% of people in the US have fluoridated tap water (14), and most water filters don’t remove the fluoride. Another downside of fluoridated water is that it can cause lead to leach from pipes into the water – some studies have found that children drinking fluoridated water have double the blood lead levels of those drinking non-fluoridated water (15). Reverse osmosis filtered tap water or bottled spring water is the best way to avoid this. So, what to do with all this information? There is no one perfect formula, just like there is no one perfect diet – what is best for your baby depends on your baby’s unique needs and what's important to you as a parent. I’ve compiled a reference chart with some of the leading options - these are not ones that I necessarily endorse, nor is it intended to be an exhaustive list, they are simply a selection of the top selling brands, plus some of the leading organic options (domestic and European), to show the variety available, and how they stack up against the criteria discussed above. 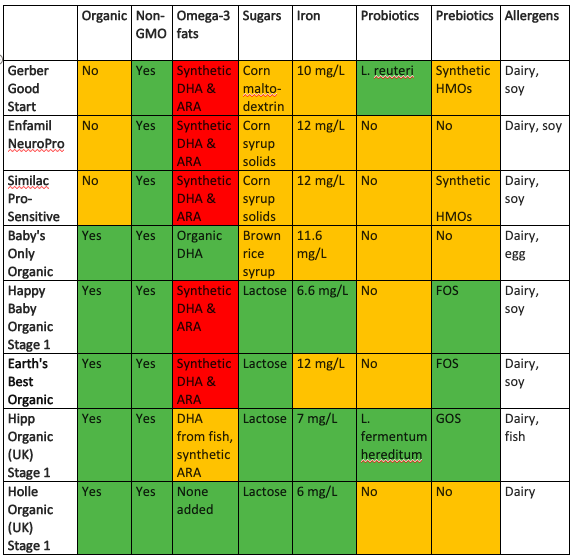 If you would like personalized guidance on what's best for YOUR baby, or to find out more about what their microbiome might be missing, please contact me, and we can set up a consultation.
1 Comment
 “What's the best type of milk for my toddler?” I get asked this question all the time, and my response is that it depends on why are you planning to give your child milk. I usually get one of these answers:
3) Don’t little kids NEED milk? It is culturally ingrained in us that our kiddos need to drink milk, and to a certain extent, this is true. Mothers’ milk is the first and best source of nourishment for an infant, and meets all of their nutritional needs for at least the first six months of life, which is pretty amazing. For the second six months of infancy, mothers’ milk is still the primary source of nutrition, with some solid foods added in for supplementary nutrients (and oral-motor development, and exploration of new tastes and textures). Historically, our babies would have continued to nurse beyond the first year, into toddlerhood and beyond, and this is still the case in most developing countries, where alternatives are not readily available. The World Health Organization (WHO) recommends that all babies nurse for the first two years of life, minimum, and after that for as long as suits the mother and child. The American Academy of Pediatrics (AAP) recommends breastfeeding for at least one year, and beyond for as long as mutually desired. In spite of this, most babies in the US don’t nurse for 12 months - in part because we have family leave policies that make breastfeeding harder to establish and maintain for working women, as well as heavily promoted alternatives (e.g. infant formula and cow’s milk). However, it may surprise you to know that while most babies in the USA aren’t still nursing at a year, more than a third of them are (36% at 12 months; CDC, 2015), and many will continue beyond this birthday into toddlerhood (1-3 years). Some women may want to introduce a supplementary milk alongside their breastmilk around the first birthday - perhaps to wean their child off the breast, or as an alternative when breastmilk isn’t available (because nobody wants to pump if they don’t have to, amirite?). Some women may decide to stop nursing at a year, and want to switch to a substitute milk. Some women may have stopped nursing sometime during the first year and switched to infant formula, and now they want to know which follow-on milk is right for their toddler. Here’s the rub: in the developed world, after the first year or so, most toddlers need milk less and less for nutritional purposes, because the majority of their nutrient requirements can be increasingly met by solid foods. This is not to say that there’s no benefit in nursing beyond a year! Human milk continues to be a convenient source of many nutrients, which can be particularly useful for picky eaters. It also continues to build the gut microbiome with beneficial bacteria which confers life-long health benefits, plus the longer a women nurses, the lower her rates of breast cancer, and this protective effect against breast cancer is also conferred to the nursing female child. And, last but by no means least, it is a great source of emotional nourishment and security for an increasingly independent child. The genius thing about human milk is that the composition adapts to meet the changing needs of your babe: from morning to night, in sickness and in health, and in different climates. This is also true over time: the fat content of breastmilk increases in the second year for growth and brain development, as do concentrations of lactoferrin (for iron absorption) and certain immunoglobulins (for extra immune support now they're more independent). Plus, in the second year, breastmilk continues to be an excellent source of B12 (94% of RDA), folate (76% of RDA), vitamin A (75% of RDA), and vitamin C (60% of RDA), and a good source of protein (43% of RDA), calcium (36% of RDA), and calories (29% of RDA). (These percentages assume 15 oz of breastmilk per day.) 2) My pediatrician said I should. Most pediatricians will tell you at the one year well-baby visit that you can start introducing cow’s milk now - that’s because you really should not give it to a baby younger than a year, as it can irritate their gut lining and cause intestinal bleeding, plus it can tax their developing kidneys, due to the higher protein content. The message from the medical team here is that after 12 months you may introduce it, rather than that you should introduce it. Remember, the majority of babies whom your pediatrician sees are likely formula-fed by their first birthday, so they may just be assuming that you’re looking for the go ahead to switch your child from formula to cows’ milk (which is much cheaper and more convenient). For breastfeeding mamas who want to continue nursing, there is absolutely no need to introduce an additional milk source to your child. Remember, all toddler milk options are substitutes for breastmilk! Water is a perfectly adequate beverage in between nursing sessions; offer freely throughout the day, especially with meals. As a precautionary tale, I have now encountered a few breastfeeding mothers who introduced cow’s milk at one year, on their pediatrician’s advice, and found that their little one ended up weaning from the breast prematurely. Some of these toddlers lost interest in breastmilk when they realized they could just get cows’ milk in a cup, whenever they wanted, and maternal supply dropped. In more than one of these cases, mothers developed mastitis due to blocked milk ducts, and this lead to terminating the breastfeeding relationship earlier than intended when antibiotics were needed. For women who have stopped nursing, or would like to, there are options:
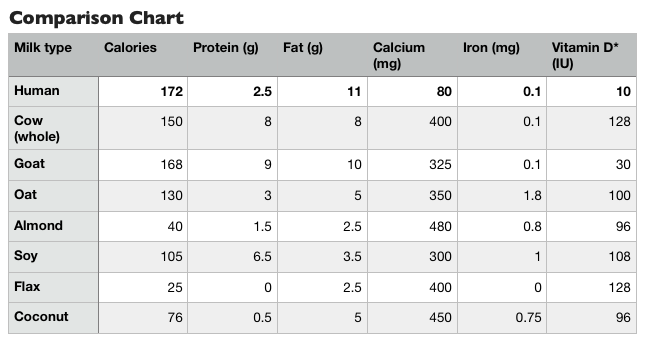 So which is closest to human milk? It depends on the nutritional category (check out the chart above). Goats' and cows' milk are the closest on calorie and fat content, but have more than three times the protein, and four to five times the calcium. This isn’t necessarily a case of more is better - remember, cow and goat milks are nature’s perfect nutrition source for baby cows and goats, not baby humans! The proteins in goats' milk are more similar to those in human milk, and overall the nutrient profile of goats' is closest to humans'. All of the plant milks are low-fat compared with mammal milks, and toddlers need adequate fat in their diets for optimal growth and brain development. The milk with the closest protein content to human milk is oat milk, and it’s also the closest in calories and fat out of the plant milks, plus it has the most iron. All of the milks have higher vitamin D content than breast milk, because it’s added by manufacturers to both cows’ milk and plant milks; you can also boost the vitamin D content of human milk with a high dose supplement (mother takes 6,400 IU per day), or supplement the child directly, per the AAP guidelines (600 IU per day). All of the milks have higher calcium content than breastmilk too - plant milks are trying to match up to cows’ milk, so they fortify with calcium to meet those levels (even if this isn’t what nature designs for human babies). Some of these alternatives are very low calorie and and don’t offer much nutrition (e.g. almond milk and flax milk). They are still more nutritious than water, so if that’s what they’re replacing in the child’s diet, then it’s likely not a problem. But, sometimes milk drinking (of all varieties) can crowd out more nutrient dense foods by filling up the child’s stomach, especially if the milks being offered are sweetened and easy to guzzle. All supplementary milk can be offered in a cup at this age, not a bottle - toddlers are developmentally ready for an open cup, and this makes milk drinking more of an intentional activity, so they’re less likely to fill up on it. Also, given the high levels of added calcium in all of the alternative milks, plus the risk of iron deficiency anemia in this age group, it is better to offer milks separately from iron-rich meals (e.g. meat and beans), as calcium inhibits iron absorption. The bottom line for all of these milk options is that none of them exactly matches the nutrition of human breastmilk, but that doesn't matter much if they are offered as part of a well balanced and varied diet of solid foods, rather than being the main source of nutrition. During the second year of life, solid foods are increasingly the main source of nutrients for the toddler, shifting from maybe 50 percent of nutrients coming from food (50 percent from milk) at one year old, to around 75 percent of nutrients coming from foods at two years old, and 90 percent or more at three years old. However, if you have a very picky eater on your hands, who is still heavily reliant on milk for nutrition, you may want to consult with a nutritionist or well-versed pediatrician on which is best for them (and trouble shoot their finicky feeding behaviors while you’re at it!).  1) How will they get enough calcium/protein/vit D without milk? I hope you now understand that none of these milks are truly necessary, just a convenient way to supplement the toddler's diet, particularly in terms of the calcium and vitamin D content. So, if your little one just isn’t into drinking milk, period, don’t sweat it - it’s not some essential elixir for them to reach their full growth potential. Calcium is important for development of strong and healthy bones, as well as muscle function, and toddlers need ~700 mg/day. Vitamin D is essential for absorption of calcium, and immune function; children in this age group (1-3 years old) need 600 IU/day. The AAP says that toddlers can get enough calcium and vitamin D each day from eight to sixteen ounces (1-2 cups) of cow's milk, or the equivalent amount of other dairy products, like yogurt or cheese. 1 cup of milk is equivalent to 1 cup of yogurt, or 1.5 oz of cheese, or 1 cup of calcium-fortified plant milk. So, if your toddler doesn’t drink milk but eats a half cup of yogurt for breakfast and a string cheese for lunch, that’s the equivalent of a cup (8 oz) of milk. Cultured dairy products like yogurt and cheese can be easier to digest, due to the fermentation process breaking down the casein proteins - many people who have a hard time drinking milk can consume yogurt and cheeses without issue, for this reason. So, if your child seems to have a slight dairy sensitivity, but not an allergy, they may have no problems with cheese and yogurt. Harder, more mature cheeses (e.g. Cheddar) are easier on the stomach than softer, younger cheeses (e.g. ricotta), as they have been cultured longer. Greek yogurt has the liquid (whey) strained out, making the protein (casein) content more concentrated, so a thinner plain yogurt or kefir can be easier to tolerate due to the lower casein content. Also, cooked/baked in milk is often fine for people with mild sensitivities, as the cooking process denatures the proteins. Really, the ‘dairy’ category is a pseudonym for calcium foods, because dairy is good source of this mineral: a cup of milk provides 300mg, half a cup of yogurt provides 200mg, 1 ounce of cheese provides ~200 mg. Other calcium-rich foods outside of the dairy family include soy products (1/2 cup of tofu, calcium fortified = 215 mg), seeds (1oz chia seeds = 180 mg), grains (1/4 of oatmeal = 45 mg), vegetables (1/4 cup of broccoli = 50 mg), and some fruits (1 dried fig = 35 mg). The AAP actually recommends limiting all milk and dairy products for toddlers, to no more than 2 cups a day for 1-year-olds, and no more than 3 cups a day for 3-year-olds, to reduce the risk of nutrient deficiencies, especially iron. Iron deficiency is fairly common in this age group, and is clearly linked with consumption of cow’s milk. Vitamin D is not typically added to dairy products other than milk, so you’d need to consider other sources of vitamin D if your child isn’t drinking a fortified milk. There aren’t very many food sources of vitamin D (we have evolved to get it from the sunshine rather than relying on food). 1 oz of sockeye salmon has around 150-250 IU (wild caught has more), and an egg yolk has around 40 IU (eggs from pasture-raised hens can have double this). Some orange juice is also fortified with vitamin D, however, fruit juices aren’t recommended for toddlers due to the high sugar content, and the fructose (fruit sugars) can cause diarrhea in tiny tummies (limit to 2-4oz if you do offer it, and dilute 50:50 with water). Vitamin D deficiency is common, due to the fact that most of us do not spend a lot of time outside, and we often protect our little ones from sun exposure when they are outside, with sun screens, hats, and protective clothing. Rickets is a condition arising from inadequate vitamin D, and calcium - bones are weakened, because vitamin D is need for calcium absorption. This condition is rare, but it is actually on the rise in some developed countries; in toddlers, the most common sign is bowing of the legs. Most milks (plant and mammal) are enriched with vitamin D, but look out for the type of D - in both fortified foods and supplements, you want vitamin D3, not D2, which your body can't really absorb. Also, vitamin D is fat-soluble, so if you’re drinking a fat-free milk fortified with D, you probably aren’t getting any of the benefits! As for protein, toddlers really don't need a whole lot. The average toddler (1-3 years old) needs around 16 grams per day to grow adequately. To personalize for your child, it's 0.55 grams of protein per pound of body weight. Two cups of cows' milk (16 oz) has 16 grams of protein. One egg has 6g, 1 oz of meat or fish has 7g (that's roughly the size of the top of your thumb). 1/4 cup of beans has ~ 4g, half a slice of bread has 1-2g, and 1 tablespoon of nut butter has ~3g. It's very easy to meet the protein needs of a toddler without milk! And, too much protein can tax their kidneys - twice the RDA is a good guide for an upper limit (1.1g/lb); for a 25 lb toddler, this would be ~25 grams protein/day. Summary:
 |
AuthorHi, I'm Amy. I'm a nutritionist in the DC area, working with clients of all ages, focusing on prenatal and pediatrics. I'm all about straightforward, evidence-based health & wellness advice - because life/parenting in the modern world is complicated enough! Categories
All
November 2022
|
Seed to Sapling Nutrition


 RSS Feed
RSS Feed